
ROADS 3.0: Revenue Benchmarking for Private Hospitals
Introducing ROADS 3.0: The Next Evolution of Revenue Benchmarking for Private Hospitals
Private hospital leaders are under growing pressure to understand where funding is aligned, where gaps may exist, and what evidence is needed before entering health fund negotiations.
That requires more than internal reporting.
It requires benchmarking that reflects the right activity, the right payer context and the right market position.
ROADS 3.0 is the next evolution of EHA’s Revenue Optimisation and Decision Support platform. It gives private hospitals a more precise way to analyse funding performance, compare activity against relevant benchmarks, understand competitive context and prepare evidence for insurer discussions.
The focus is simple: clearer insight, stronger preparation and better-informed commercial decisions.
From benchmark reporting to revenue intelligence
ROADS has always been designed to help hospitals understand how funding compares to benchmarks.
ROADS 3.0 takes that further.
The platform now provides hospitals with more granular ways to analyse admitted activity, isolate acute care performance, compare HCP and PHDB benchmark views, review DRG version impacts, map competitor contracting patterns, and export filtered data for further analysis.
For CEOs, CFOs and contracting teams, this matters because the negotiation question is rarely simple.
It is not just:
What were we paid?
It is:
How does that funding compare to the relevant market benchmark, and where is the commercial opportunity concentrated?
That is the question ROADS 3.0 is built to support.
Enhanced benchmarking: Isolating acute care performance
A major upgrade in ROADS 3.0 is enhanced HCP benchmarking, using only acute care-type admissions.
This matters because all-admissions benchmarks may include activities that do not reflect the specific contracting question hospital leaders are trying to answer.
The Department’s preliminary 2024–25 HCP and PHDB annual reports now include two versions of the AR-DRG table: one based on all separations and one based on acute separations only. The acute-only version excludes admitted sub-acute, non-acute and mental health activity.
ROADS 3.0 allows hospitals to apply this acute-care lens inside the platform.
That gives leadership teams a cleaner way to assess acute care revenue performance and understand how results shift when different activity types are included or excluded.
This is particularly important when a hospital needs to understand whether an apparent gap is driven by pricing, activity mix, care type, insurer behaviour or benchmark scope.
HCP and PHDB: Why both views matter
ROADS 3.0 continues to support benchmarking using both the Hospital Casemix Protocol and the Private Hospital Data Bureau annual report.
These datasets are related, but they do not answer the same question.
HCP data is submitted by hospitals to health insurers, who then supply it to the Department. It covers admitted hospital treatment episodes where health insurers have paid a benefit.
PHDB data is submitted directly by private hospitals to the Department. It includes private hospital episodes paid by individuals and private health insurers, as well as hospital charges for all private hospital patients.
For contract preparation, this distinction matters.
HCP can provide a more insurer-aligned view of privately insured admitted activity.
PHDB can provide a broader view of private hospital activity submitted by providers.
ROADS 3.0 helps hospitals compare these perspectives, rather than relying on a single benchmark that may not reflect the commercial question being asked.
Questions ROADS 3.0 helps hospitals answer
The enhanced benchmarking capabilities are designed to help hospital teams answer more specific commercial questions, including:
Is our funding aligned with insurer-view benchmarks or broader provider-market benchmarks?
Where does the funding gap appear to be concentrated?
How does our acute care activity compare when separated from sub-acute and non-acute activity?
How do results shift when self-funded or other non-PHI activity is included?
Which services, DRGs, contracts or insurers should be prioritised before the next negotiation?
These are not only technical questions.
They are executive questions.
They affect revenue strategy, contracting priorities, board reporting and negotiation preparation.
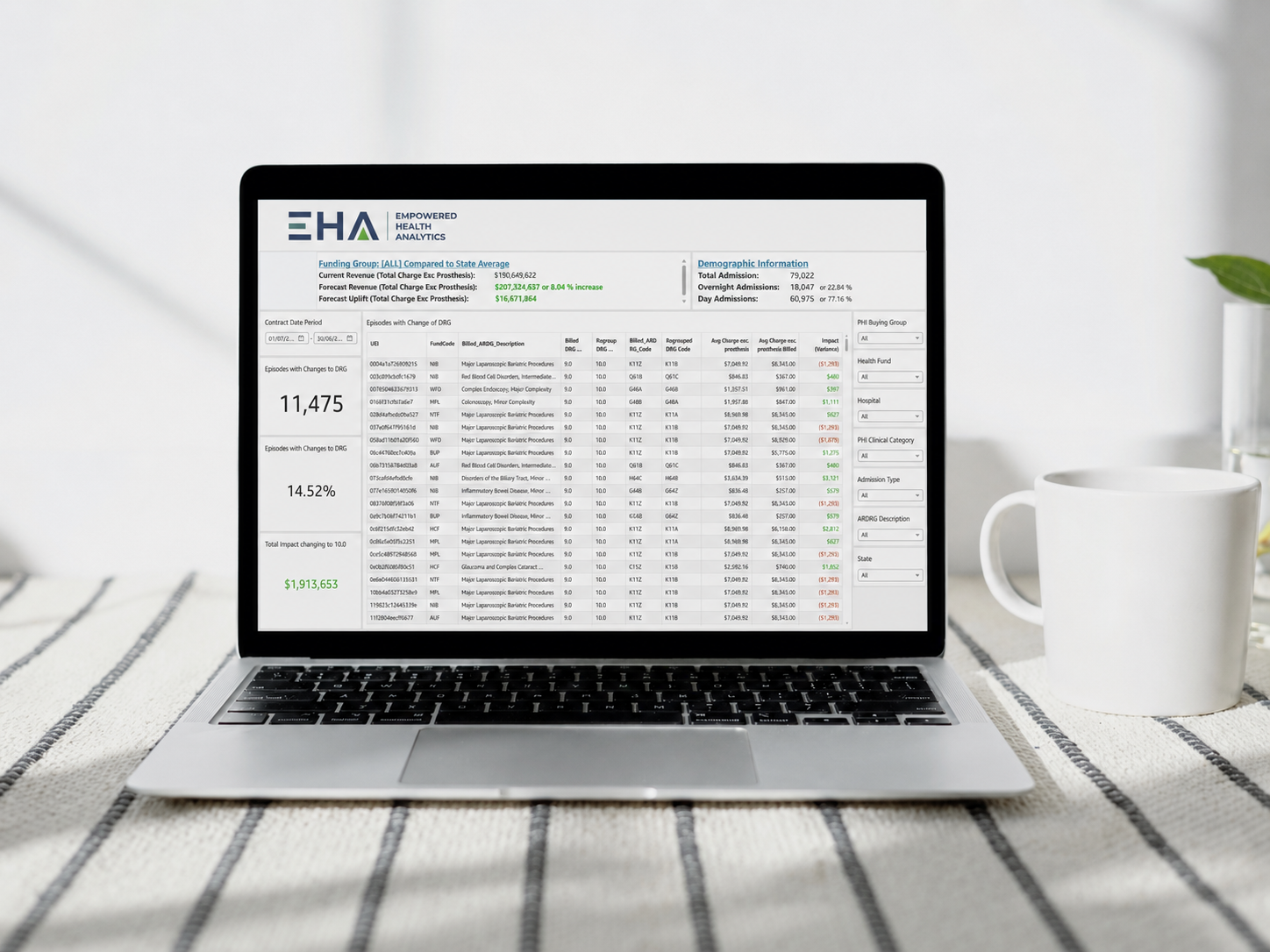
Dynamic DRG regrouping
Different funders may use different DRG versions, which can make contract analysis difficult to interpret.
ROADS 3.0 introduces dynamic DRG regrouping, enabling hospitals to assess how activity and revenue opportunities may shift across different DRG versions.
The module allows users to compare billed AR-DRG codes with regrouped DRG codes, review current and forecast revenue, quantify potential uplift and identify which episodes are affected.
The analysis can also be filtered by funder, hospital, clinical category, admission type, AR-DRG description and state.
This helps hospitals move beyond broad averages and understand the financial impact of DRG version changes at a more practical level.
For finance, coding and contracting teams, this provides a clearer view of where the impact sits before strategic or operational decisions are made.
Integrated competitor analysis map
Health fund negotiations do not happen in isolation.
Hospitals need to understand their own position, as well as the broader market context around them.
ROADS 3.0 includes an integrated competitor analysis map that helps hospitals understand where peer hospitals are located and how contracting status may vary across funders.
This gives leadership teams a clearer view of the local and regional contracting context.
That visibility can support negotiation preparation, market assessment and board-level discussion about competitive position.
Integrated data extract tool
ROADS provides visual analysis, but many finance and analytics teams still need exportable data for internal reporting, modelling or board packs.
The new integrated data-extraction tool enables hospitals to download filtered datasets from the platform.
That means teams can take enhanced data cuts from ROADS and use them in their own analysis tools, BI environments or internal reporting templates.
The value here is practical.
ROADS becomes not only a platform for insight, but a source of structured evidence that can be used across the hospital’s existing reporting workflows.
Built-in user guide videos
ROADS 3.0 also includes a built-in suite of user guide videos.
These tutorials are designed to help hospital teams understand platform features, apply filters, interpret outputs and use the system more confidently.
For busy teams, this matters.
Better guidance means faster adoption and less reliance on a few internal power users.
Why ROADS 3.0 matters for private hospital leaders
Private hospitals are operating in a contracting environment where internal reporting is no longer enough.
Leadership teams need to know not only what happened, but whether current funding is aligned with benchmarks and where a material opportunity may exist.
ROADS 3.0 supports that shift.
It helps hospitals move from fragmented data and broad averages to more precise benchmarking, clearer market context and negotiation-ready evidence.
For CEOs, CFOs and contracting teams, the benefit is not simply more data.
It is a clearer basis for decision-making before the next insurer discussion.
The takeaway
ROADS 3.0 gives private hospitals a more precise way to understand revenue performance and contracting position.
With acute-care benchmarking, HCP and PHDB comparison, DRG regrouping, competitor mapping, data extract tools and user guide videos, the platform helps hospitals turn funding data into practical commercial insight.
In a market where health fund negotiations depend on evidence, hospitals need more than assumptions.
They need a clear view of their position, the market context and the opportunity in front of them.
See your revenue opportunity
EHA helps private hospitals identify funding gaps, quantify revenue opportunities and strengthen insurer negotiations through independent benchmarking, ROADS analytics and advisory support.
Start with a confidential Complimentary Benchmark Review to determine whether your health fund contracts are aligned with the benchmark.
FAQs
-
ROADS 3.0 is the latest version of EHA’s Revenue Optimisation and Decision Support platform. It helps private hospitals benchmark funding performance, analyse revenue opportunity and prepare evidence for private health insurer negotiations.
-
ROADS 3.0 includes enhanced acute-care benchmarking, dynamic DRG regrouping, an integrated competitor analysis map, a data extract tool and built-in user guide videos.
-
Acute-care benchmarking helps hospitals separate acute admitted activity from sub-acute, non-acute and mental health activity. This can provide a cleaner view of acute care revenue performance and reduce distortion from mixed activity types.
-
ROADS supports benchmarking using both HCP and PHDB annual report data. HCP gives an insurer-aligned view of admitted episodes where health insurers paid a benefit, while PHDB gives a broader private hospital view that includes episodes paid by individuals and private health insurers.
-
ROADS helps hospitals understand where funding may sit below benchmark, where potential opportunity is concentrated and what evidence can support executive review and insurer discussions.